Introduction
Pratitioners in the emergency department frequently encounter patients who have sustained trauma to the sole of the foot and require anesthesia for repair. This tender area is relatively difficult to anesthetize locally. Regional block of the posterior tibial nerve allows for rapid anesthetization of the heel and plantar regions of the foot. Regional blocks have several advantages compared to local infiltration, such as fewer injections necessary to attain adequate anesthesia, smaller volume of anesthetic required, and less distortion of the wound site. Because of the lower number of injections, this procedure is better tolerated by the patient and limits the chance of a needle stick to the provider.
This procedure, often overlooked in the emergency department, is safe, relatively easy to perform and can provide excellent anesthesia to the foot. In one study, regional anesthesia of the foot and ankle, when performed by surgeons, was completely successful 95% of the time.
Anatomy
Understanding the arborization of the tibial nerve is crucial to a successful posterior tibial nerve block. The posterior tibial nerve arises from the sciatic nerve and courses down the posterior thigh and posteromedial lower leg, as shown below.

The tibialis posterior tendon, flexor digitorum tendon, posterior tibial artery, posterior tibial nerve, and flexor hallucis longus tendon at the ankle level.
These nerves supply the intrinsic muscles of the foot, excluding the extensor digitorum brevis. They also supply sensory innervation to the plantar surface of the foot, shown below.

Cutaneous innervation by the medial and lateral branches of the posterior tibial nerve.
At the level of ankle, the posterior tibial nerve can be found midway between the medial malleolus and the heel. The nerve lies beneath the flexor retinaculum between merging tendons and vessels. A common mnemonic is T om, D ick, AN d H arry, which correlates with the anterior to posterior progression of T ibialis posterior tendon, flexor D igitorum tendon, posterior tibial A rtery, posterior tibial N erve, and flexor H allucis longus tendon.
Indications
- Wound repair or exploration of the calcaneal or plantar regions of the foot
- As part of an ankle block required to manipulate a fractured or dislocated ankle (A combination of posterior tibial, saphenous, superficial peroneal, deep peroneal, and sural nerve blocks results in complete block of sensory perception beneath the ankle, as pictured below.)
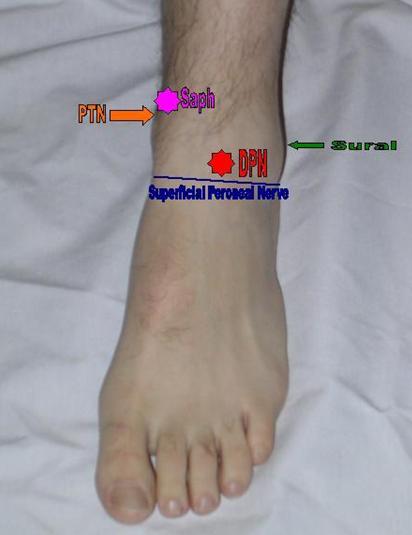
Areas of anesthetization to complete an ankle block. This block requires anesthetization of 5 nerves for complete sensory block below the ankle.
The areas to anesthetize include a line along the anterior ankle for the superficial peroneal nerve (blue line), the deep peroneal nerve (red star), the saphenous nerve (pink star), the sural nerve (green arrow), and the posterior tibial nerve (orange arrow).
- Relief of tarsal tunnel syndrome
- Incision and drainage of an abscess in the calcaneal or plantar regions of the foot
- Foreign body removal in the calcaneal or plantar regions of the foot
Contraindications
- Allergy to anesthetic solution or additives (eg, ester, amide)
- Injection through infected tissue
- Severe bleeding disorder or coagulopathy
- Preexisting neurological damage
- Patient uncooperativeness (Pediatric or elderly patients may need sedation.)
Anesthesia
- The 2 main classes of local anesthetics currently in use are amino esters and amino amides. Both inhibit ionic fluxes required for the initiation and conduction of nerve impulses. Lidocaine, the most commonly used anesthetic, has a fast onset of action and a duration of action of 30-120 minutes, which is increased to 60-400 minutes with the addition of epinephrine.
- The total cumulative dose of lidocaine to be infiltrated is 5 mg/kg (not to exceed 300 mg) if lidocaine without epinephrine is used, and 7 mg/kg (not to exceed 500 mg) if lidocaine with epinephrine is used.
- Anesthetic preparations that contain epinephrine are commonly used in the emergency department. Epinephrine induces vasoconstriction, decreasing the amount of local bleeding at the site of injection. In addition, it increases the duration of action of the anesthetic with which it is combined. Despite these advantages, the vasoconstrictive properties of epinephrine may contribute to tissue hypoxia, and its use should be avoided in areas of poor perfusion (ie, fingers, toes, penis, ears, nose).
- Topical anesthetics may be needed in children or uncooperative adults.
Equipment
- Needle, 4 cm, 25 gauge (ga)
- Needle, 18 ga
- Syringe, 10 mL
- Marking pen
- Sterile gloves
- Antiseptic solution (eg, povidone iodine [Betadine], chlorhexidine gluconate [Hibiclens]) with skin swabs
- Alcohol swabs
- Sterile drape
- Lidocaine 1%, 10 mL
- Facial mask with eye shield
- Sterile gauze

Equipment needed for the regional block.
Positioning
- Position the patient supine and as comfortably as possible.
- Alternatively, the patient may sit and face the physician.
Next >> Technique
Source Emedicine.medscape.com
Originally posted 2010-09-18 04:23:28.
